 The following data and information were collected and analyzed by Tracey P. Lauriault, and Sam Shields a recent Carleton University Critical Data Studies graduate.
The following data and information were collected and analyzed by Tracey P. Lauriault, and Sam Shields a recent Carleton University Critical Data Studies graduate.
We set out to answer a very simple question inspired by a Twitter stream calling for COVID-19 reporting to include Indigenous, Black and Racialized characteristics. The following guided our activities:
- What kind of demographic data are reported in official COVID19 reports?
On Thursday April 16, 2020 we spent the day searching the content of official government COVID-19 reporting sites. We compiled our data into a Google Spreadsheet, conferred over Skype, chatted in FB, and verified each other’s work. Official COVID-19 reporting dynamically changes as the pandemic evolves, and as institutions collect more data and build the capacity to report, they report more and they do so in a better way. I also consult experts in my network who comment and suggest resources. We will take another look next week to see if anything has changed. The following were our data sources
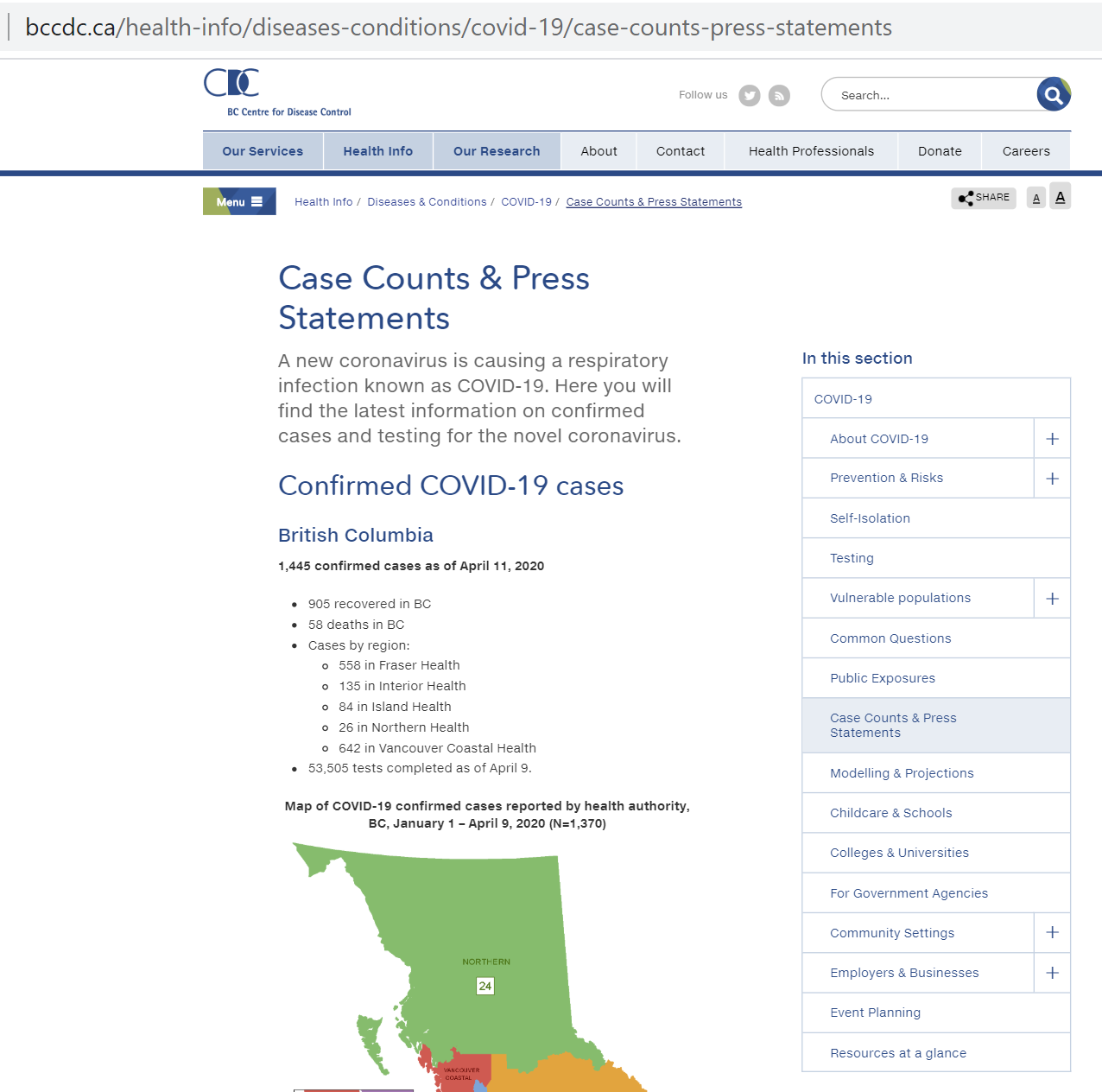
- British Columbia: COVID Dashboard & BCCCD PHSA Surveillance Report (15/04/2020)
- Yukon: Information about COVID-19
- Alberta: COVID-19 in Alberta
- North West Territories: Coronavirus Disease (COVID-19)
- Saskatchewan: Cases and Risk of COVID-19 in Saskatchewan
- Manitoba: COVID-19 Updates
- Nunavut: COVID-19 (Novel Coronavirus)
- Ontario: The 2019 Novel Coronavirus (COVID-19) Status of cases in Ontario & Daily Epidemiologic Summary (15/04/2020)
- Québec: Données COVID-19 au Québec & Situation du coronavirus (COVID-19) au Québec
- New Brunswick: COVID-19 Testing by the Numbers
- Prince Edward Island: PEI COVID-19 Testing Data
- Nova Scotia: Novel coronaviris (COVID-19) cases in Nova Scotia: data visualization
- Newfoundland: Newfoundland and Labrador Pandemic Update Data Hub
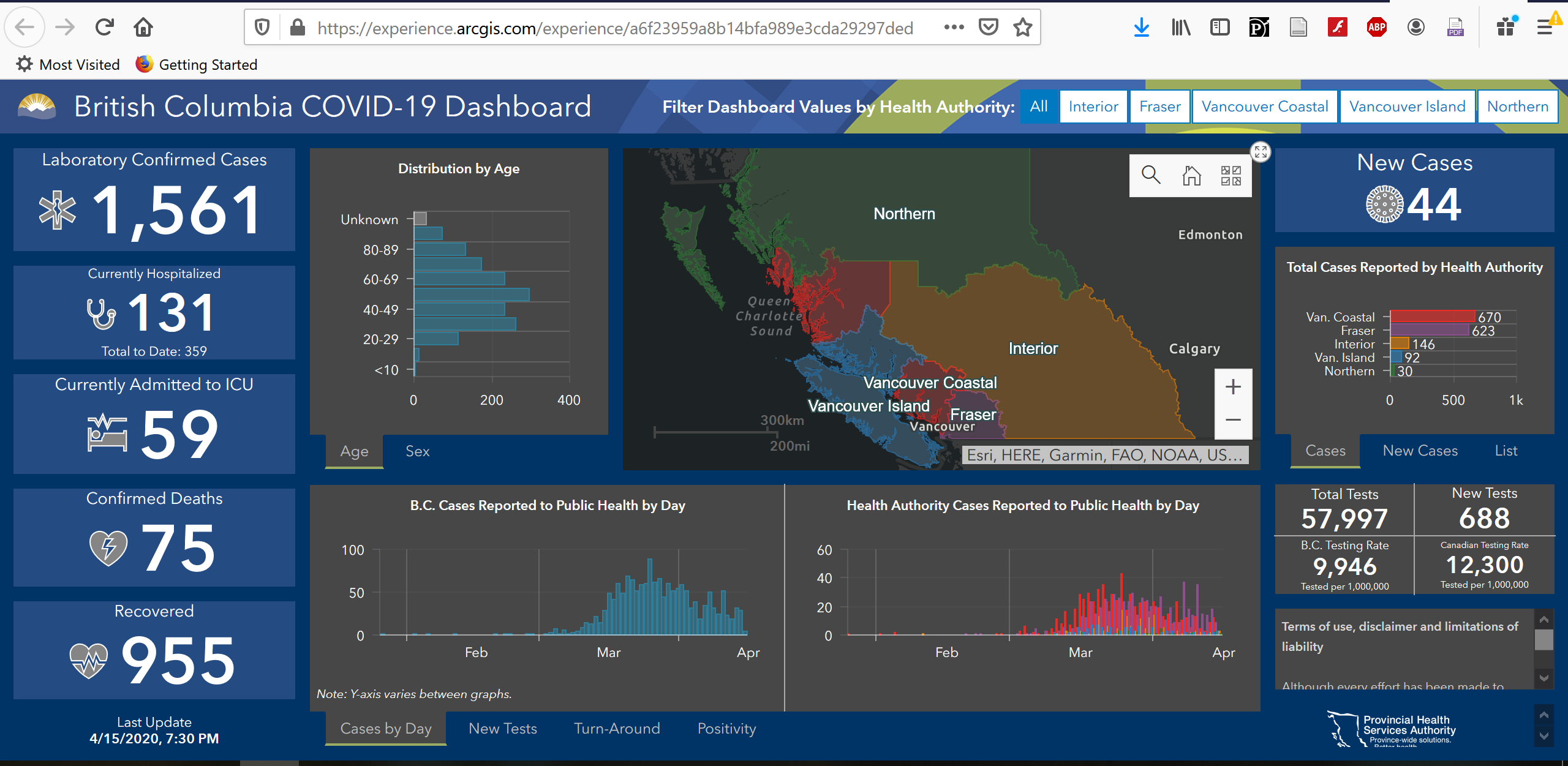
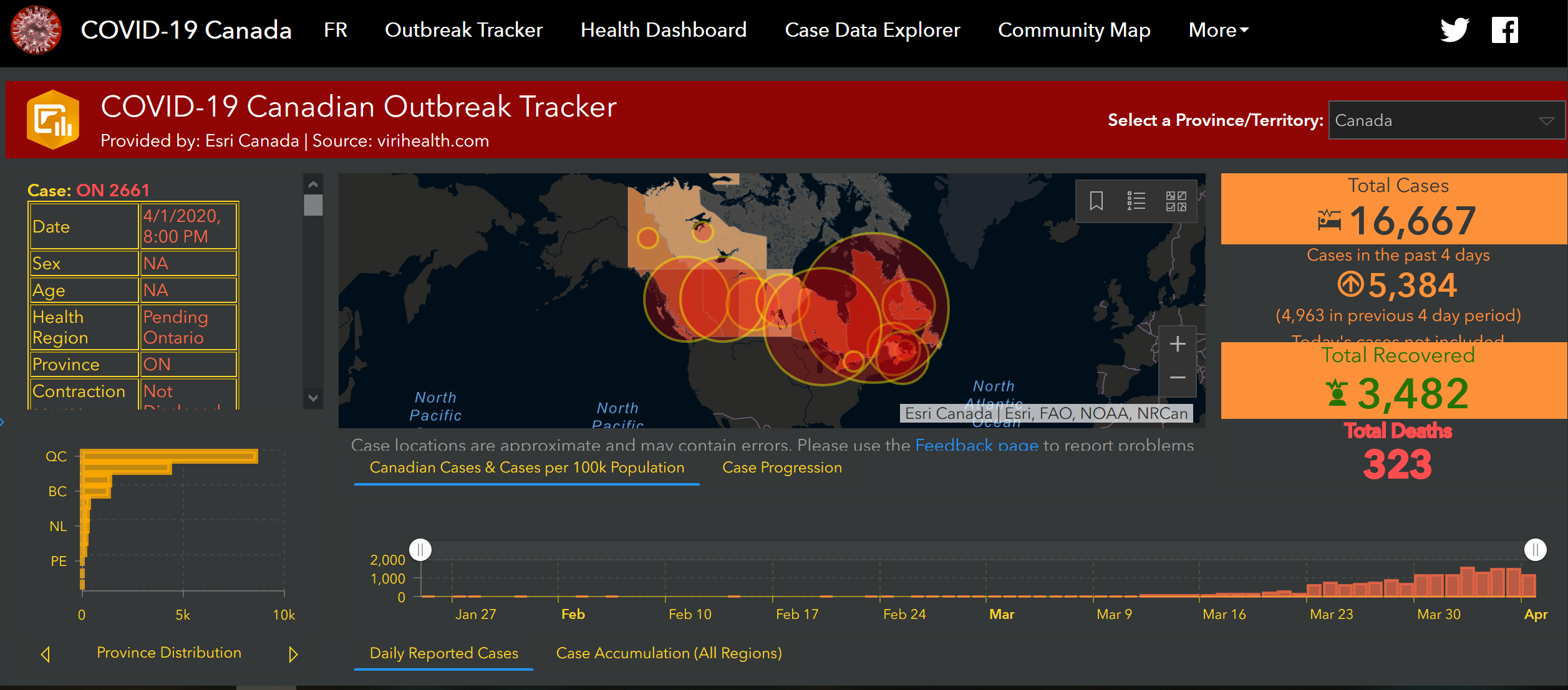
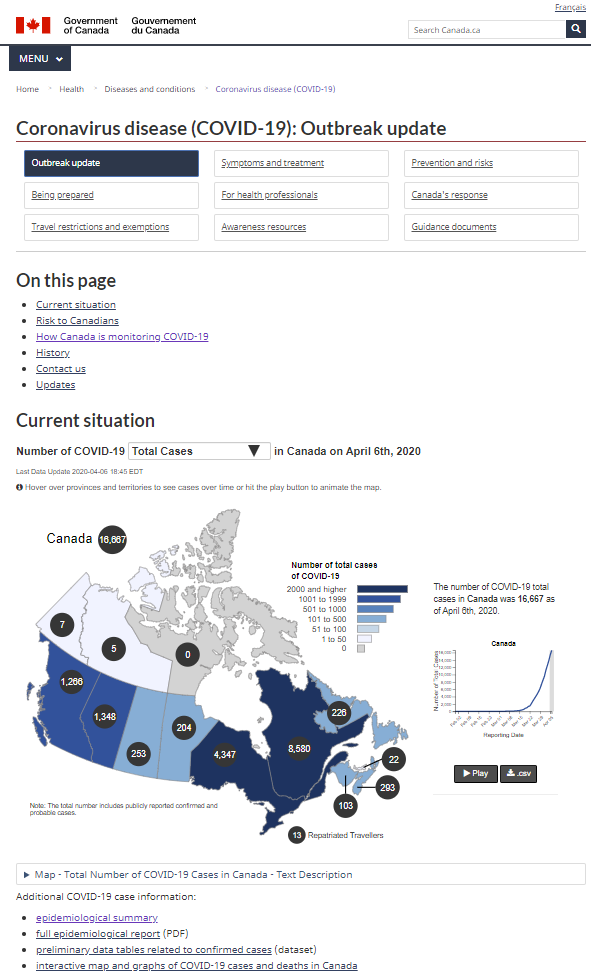
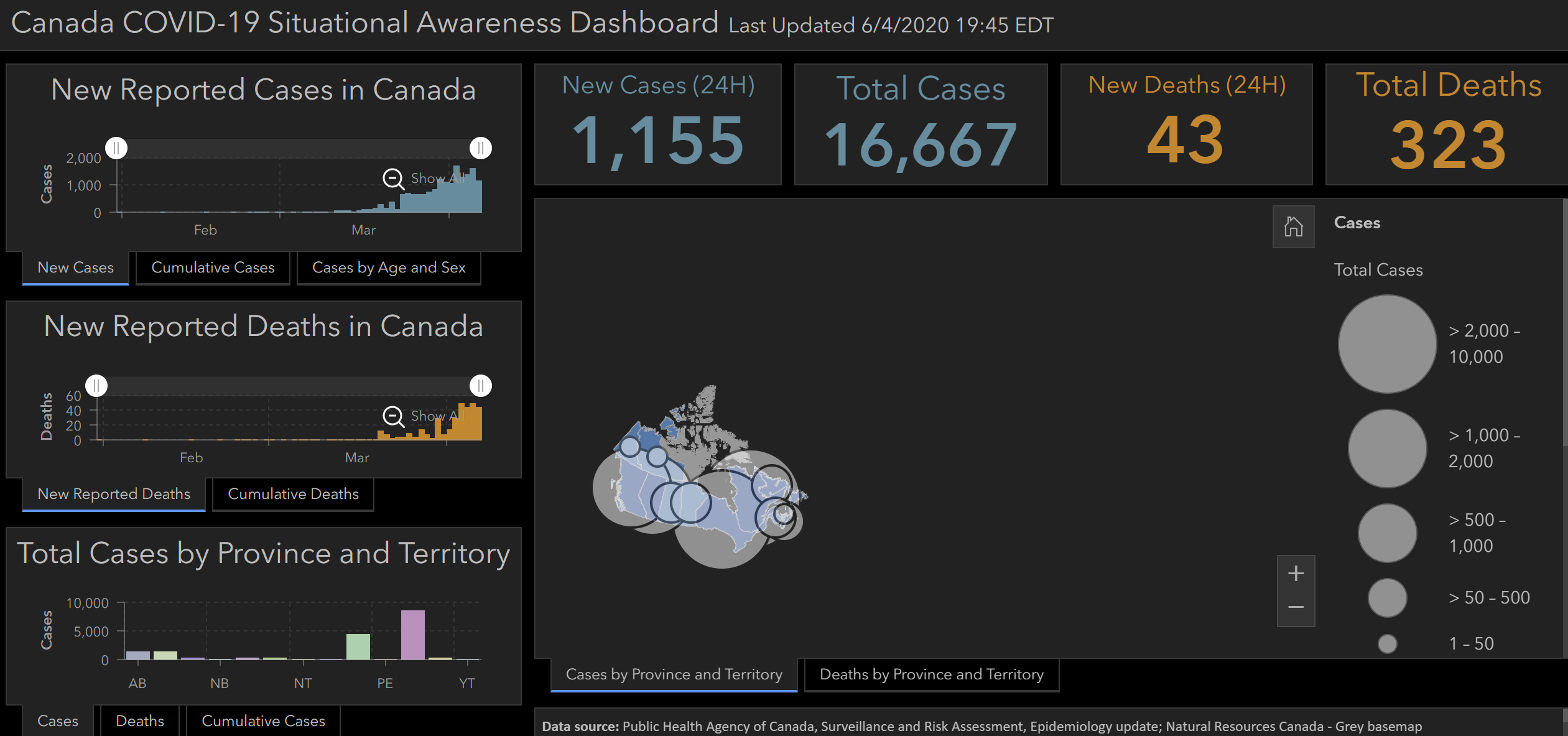
- Federal: PHAC Coronavirus disease (COVID-19): Outbreak update & Full Daily Epidemiology Update (April 16, 2020)
We found an incredible amount of information and overall, each province, territory and the Federal government make their data readily available and these are disseminated in charts, tables, maps, and dynamic dashboards and in daily surveillance reports. The data and indicators are explained, and data sources are generally provided.
In terms official COVID-19 reporting, there was very little reporting cases and outcomes with demographic variables and when there was, it is not standardized, making it difficult to do any national comparative analysis. Below is what we found.
1. Age
- COVID-19 Cases by Age were reported by all provinces and the Federal Government. Age was not reported by all 3 Territories.
- Those who did report, provided case counts and some percentages.
- Only British Columbia, Alberta and Quebec reported Deaths by age groups.
- Quebec reports age in 4 different ways.
- There are no Age Range Reporting standards, and this impedes comparability.
The following is how COVID-19 Age data are reported, we ordered the results by similar reporting styles.
- British Columbia: <10, 10-19, 20-29, 30-39, 40-49, 50-59, 60-69, 70-79, 80-89, 90+, Unknown
- New Brunswick: <10, 10-19, 20-29, 30-39, 40-49, 50-59, 60-69, 70-79, 80-80, 90+
- Manitoba: 0-9, 10-19, 20-29, 30-39, 40-49, 50-59, 60-69, 70-79, 80-89, 90-99, 100+
- Quebec: 0-9, 10-19, 20-29, 30-39, 40-49, 50-59, 60-69, 70-79, 80-89, 90+, Unknown
- 0-29, 30-39, 40-49, 50-59, 60-69, 70-79, 80-89, 90+
- 30-49, 50-69, 70-79, 80-89, 90+
- <30, 30-39, 40-49, 50-59, 60-69, 70-79, 80-89, 90, Unknown
- Alberta: <1, 1-4, 5-9, 10-19, 20-29, 30-39 ,40-49, 50-59, 60-69, 70-79, 80+
- Saskatchewan: <19, 20-44, 45-65, 65+
- Ontario: <19, 20-39, 40-59, 60-79, 80+
- Federal: 19, 20-29, 30-39, 40-49, 50-59, 60-69, 70-79, 80+
- Nova Scotia: 0-19, 20-44, 45-64, 65+
- PEI: <20, 20-39, 40-59, 60-79, 80+
- Newfoundland: <20, 20-39, 40-49, 50-59, 60-69, 70+
- Yukon: No Reporting by Age
- North West Territories: No Reporting By Age
- Nunavut: No Reporting By Age
Age range variable reporting recommendations:
a) Standardize age ranges reporting systems across jurisdictions to enable comparison.
b) Social-determinant of health variables, such as occupation, income, the type of dwelling a person lives in, where one lives, are variables being reported as being related to COVID-19. The Census reports age by quintile although it start at 0-14, in Canada vital statistics are reported by age quintile and the World Health Organization (WHO) also reports by quintile. Linking to other aggregated demographic, health and vital statistical data can inform the planning, and the managing of health outcomes.
2. Sex
- Sex is Not reported as a COVID-19 attribute, by 4 Canadian jurisdictions, namely the Territories and Newfoundland and Labrador.
- For jurisdictions that do report COVID-19 data by sex, only binary classifications are used, Female and Male.
- Only British Columbia, Alberta and Manitoba report Sex and Age as attributes.
- Only Quebec and The Federal Government report Sex and Death.
Sex Variable Reporting Recommendations:
a) It is advisable to report COVID-19 indicators by sex such as Female, Male and Gender Diverse.
b) Sex disaggregated data are important in terms of informing testing; health interventions and it is associated with health outcomes. Knowing can inform planning.
c) Reporting age and sex is important as these are distinguishing characteristics in vital statistics, health, wellbeing, for longevity and death rates. Also, reports suggest that the virus affects men more negatively than it does women, especially older men. In terms of the labour force and COVID-19, nurses, doctors, elder care and home care professionals, those who work with people who live in group homes for the disabled and provide home care for these people, and people who clean these places tend to be women. Higher numbers of women are becoming afflicted by COVID-19 in Canada and this may be associated with their occupations. Age and sex are standard labour force statistical variables and reporting these attributes with COVID-19 will inform if health outcomes are related to those attributes.
3. Labour Classification
- In official COVID-19 reporting, only the Provinces of Saskatchewan and Quebec reported any labour category and respectively they reported Case Counts for Health Care Workers for Saskatchewan and Cases Count and Death Count of Staff in hospitals and long-term care homes for Quebec.
Labour Force Reporting Recommendations:
a) Canadian Labour Forces Characteristics such as employed full or part-time, and the North American Industry Classification System and National Occupation Classification (NOC) system are standardized. For example, see the NAICS Health Care and Social Services or the classification and search for cleaner in NOCS.
b) The Canadian Institute for Health Information (CIHI) health workforce database includes standardized job classifications and data tables by job classification. They also have methodological guides comparing provincial systems. Harmonizing classifications across the provinces and the territories would go a long way to facilitating comparable analysis.
4. Indigenous, Black and Racialized People
- No official government COVID-19 sites report data by any of these groups.
- Race and ethnicity may or may not biologically predispose people to COVID-19 health outcomes. We are assuming that these data are being tracked but are not reported as there is a concern about how to report these data.
- Indigenous, Black and Racialized people may also have preexisting health conditions that are socially and economically determined, and these preexisting conditions may disproportionally affect this group more than others. Furthermore, reports suggest that Indigenous, Black and Racialized People have been infected more than others, and their health outcomes are more dire. Evidence informed decisions can lead to better outcomes for some groups, reporting the numbers can advance better and more targeted practices in community, hospital and in our cities.
Recommendation on the Reporting with Indigenous, Black and Racialized People categories:
a) The Province of Ontario Anti-Racism Directorate publishes a Data Standards for the Identification and Monitoring of Systemic Racism that includes
“guidance for race-based data collection for government and other public sector organizations, including steps to follow for data collection, management and use”.
Table 1. Valid Values for Race Categories on P.26 provides a useful classification system. The Standard also includes protocols for the collection of self reported or observed data.
b) First Nation, Metis and Inuit in Canada may be collecting these data in their communities. I will consult to see if that is the case and report back.
Final Remarks:
Health outcomes are intersectional, and age, sex, workforce and equity data provided additional insight about who is being affected, and knowing who and where can inform decisions about determinants of health, testing, improvement of health outcomes and planning. We have provided some insight in this post, about what is being reported and provided some recommendations. We will provide updates as more information is collected. We hope you find this useful and we welcome your comments and suggestions by email: tracey.lauriault@carleton.ca or on Twitter @TraceyLauriault.

Comments on Posts